You’re doing what you’ve always done, walking more, eating “pretty well,” maybe even skipping dessert, and yet your waistline still feels different. If you live in Chicago, you might notice it most in January, when layers hide the change until you catch your reflection, then it hits you all at once. Belly fat can seem to show up overnight in perimenopause or menopause, and it can feel personal, even when it’s not.
Here’s the truth you deserve upfront: HRT can help with the hormone-driven shift toward belly fat, and it can improve sleep, energy, and joint comfort. But HRT is not a weight-loss drug. This article splits things clearly into what research supports, what it doesn’t, and what helps most for Weight Loss and waist size in midlife.
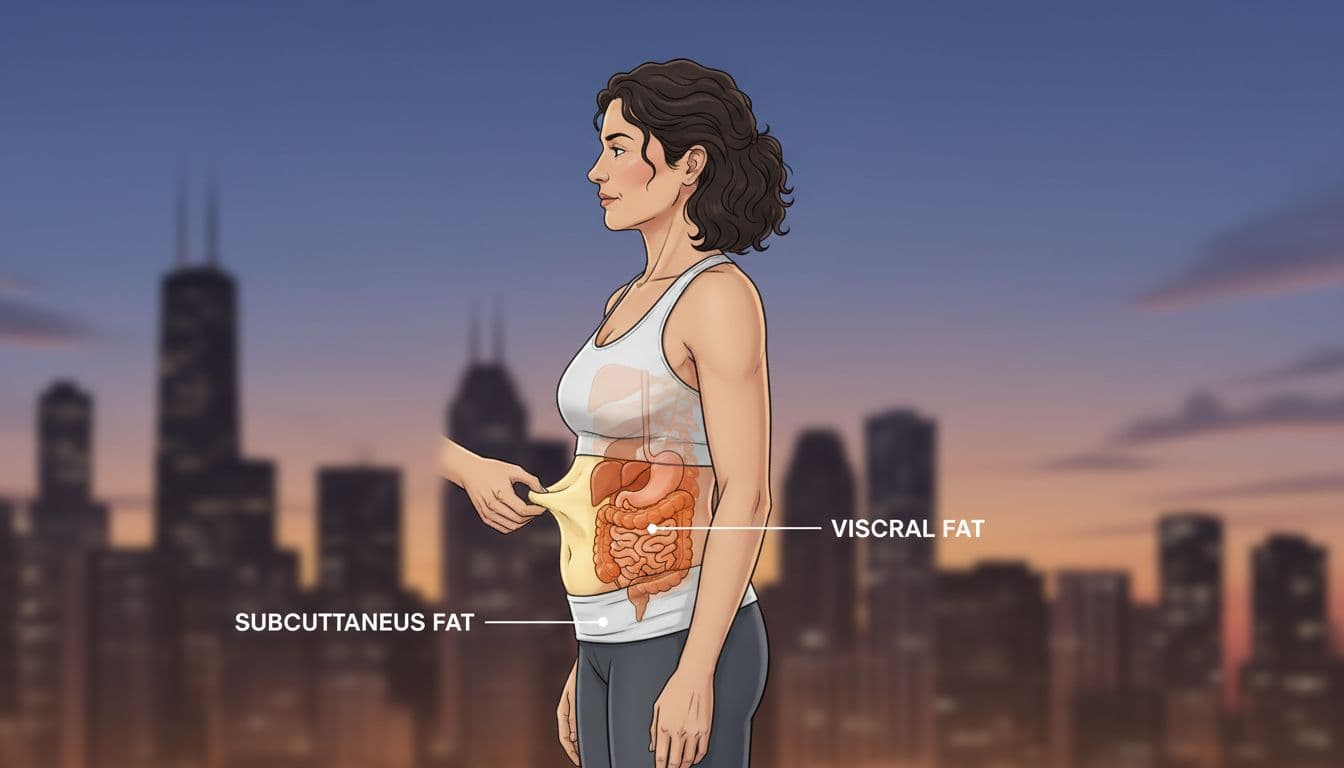
When people say “belly fat,” they often mean two different things: the pinchable layer under your skin (subcutaneous fat) and the deeper fat around your organs (visceral fat). Visceral fat matters more for heart health and blood sugar, even if it’s less obvious in the mirror.
If you’re still sorting out where you are in the transition, this guide on Differences Between Perimenopause and Menopause can help you make sense of what’s normal and what isn’t.
Why belly fat shows up in perimenopause and menopause (and why it feels so unfair)
Midlife belly changes usually come from a stack of forces that hit at the same time: lower estrogen, normal aging, muscle loss, sleep disruption, and more insulin resistance. Even if your diet hasn’t changed much, your body can start storing fat differently.
A frustrating part is that your waist can grow even when the scale barely moves. That’s body composition shifting, less muscle, more fat, and more of it moving toward your midsection.
Here’s the plain-language breakdown:
Type of belly fatWhere it sitsWhy it mattersSubcutaneous fatUnder the skin (pinchable)Affects how your clothes fit, less tied to metabolic riskVisceral fatDeeper, around organsStronger link to blood sugar, cholesterol, and heart risk
The estrogen drop can shift fat storage toward your midsection
As estrogen declines, research consistently shows a stronger tendency toward central fat storage. You’re not imagining the “apple-shape” shift. Your body becomes more likely to store fat around the waist after menopause, sometimes even without big diet changes.
This doesn’t mean you’re doing anything wrong. It means the rules changed.
Loss of muscle lowers your daily calorie burn
Muscle is like your metabolic engine at idle. When you lose it, your body burns fewer calories at rest. That’s one reason Weight Loss can feel slower now, and it’s also why strength training matters so much for your waistline.
HRT and belly fat, what science supports (and what results are realistic)
The strongest takeaway from research through 2025 is simple: hormone therapy can slow or partly prevent the usual gain in abdominal fat after menopause, especially visceral fat gain. But most women won’t see dramatic weight drops from HRT alone.
In many studies, the scale changes little. What can change is how fat is distributed, often a smaller increase in waist size and a better waist-to-hip ratio compared with no HRT.
If you want a deeper explanation of what you might see on the scale versus in your waist, read How HRT Affects Weight and Belly Fat.
HRT may help prevent visceral fat gain, more than it causes major weight loss
It helps to think of HRT like a seat belt for menopause body changes. It can reduce the “impact” of the shift toward belly fat, but it doesn’t melt fat off your body. Studies and reviews often show modest improvements in abdominal fat measures and waist size, not big, fast Weight Loss.
The most realistic win is prevention: less new belly fat gain over the next year or two, compared with what might happen without treatment.
Why you might feel better on HRT and then lose weight more easily
This is where HRT can shine as a support tool. If hot flashes ease, night sweats calm down, and your mood steadies, your habits get easier to repeat.
Better sleep can mean fewer cravings. Less joint pain can mean more walking. More energy can mean you cook instead of graze. The habits still drive fat loss, but HRT can remove the roadblocks that kept you stuck.
What HRT doesn’t do, and common reasons your belly still won’t budge
HRT is usually prescribed for symptom relief (hot flashes, sleep, vaginal symptoms, quality of life), not as a primary Weight Loss treatment. It also doesn’t work the same for everyone, and the type, dose, and route can change how you feel.
Belly fat can also hang on for reasons that have nothing to do with your hormones. Common ones include:
- Alcohol (even “just a couple” most nights)
- Ultra-processed snack foods
- Low protein intake
- Low daily movement
- Poor sleep and high stress
- Certain meds (some antidepressants, steroids, and others)
- Untreated thyroid issues or rising A1C (blood sugar)
HRT can’t outwork ultra-processed snacks, alcohol, and low protein
You don’t need perfect eating, but you do need a pattern that supports your goals. Ultra-processed foods make it easy to overshoot calories without feeling full. Alcohol adds liquid calories and often worsens sleep, which can push cravings the next day.
Low protein is a quiet problem in midlife. If you don’t eat enough protein, you’re more likely to lose muscle during Weight Loss, and that makes long-term results harder to keep.
Bloating and water retention can look like “belly fat” at first
Early on, some people feel puffy on HRT. That’s often fluid shifts, not fat gain. Clues it’s water include rapid changes over days, tighter rings, and a general “swollen” feel.
Instead of judging your body by one morning mirror check, track your waist measurement and how your jeans fit over several weeks. Fat loss is slow, water changes are fast.
What helps most for belly fat and weight loss during menopause (with or without HRT)
Your best food strategy: protein at each meal, high fiber, fewer liquid calories

Build meals the way you’d build a sturdy house: start with the frame.
Start with protein, then add fiber and color. Practical options include eggs, Greek yogurt, fish, chicken, tofu, beans, and lentils. Add fiber from veggies, fruit, oats, and beans, and include healthy fats (olive oil, nuts, avocado) to stay satisfied.
A gentle calorie gap (often 300 to 500 calories per day) is usually more sustainable than crash dieting. Extreme diets can shrink muscle fast, and that can make your belly look softer over time.
Your best exercise strategy: lift weights, then add cardio and more daily steps
For belly fat, strength training is your anchor. Aim for 2 to 3 days per week, focusing on big moves: squats, hinges (deadlift-style), pushes, pulls, carries, and planks. Start light, and keep showing up.
Then add cardio. Many women do well with about 150 minutes per week of moderate activity (like brisk walking), plus a daily step goal you can actually hit in real life (often 7,000 to 10,000 steps). In Chicago winters, indoor mall walks, stairs, or treadmill incline walks count.
Sleep and stress can drive belly fat, fix these and fat loss gets easier
When sleep breaks down, hunger hormones and cravings ramp up. Stress can also push comfort eating and make workouts feel harder to start. The result is a calorie surplus that sneaks in.
A short sleep checklist that works:
- Keep a steady bedtime and wake time most days
- Sleep in a cool, dark room
- Get morning light when you can
- Cut late caffeine, and watch alcohol near bedtime
- Do a short wind-down (stretching, reading, slow breathing)
- Take a 10-minute walk when stress spikes
If HRT reduces night sweats, your sleep often improves, and consistency gets easier.
When to ask about prescription weight-loss meds, and how they may pair with HRT
If you’ve tried for months, and your hunger feels louder than your plan, it may be time to talk about prescription options. GLP-1 meds (and newer GIP/GLP-1 options like tirzepatide) can produce meaningful Weight Loss for some women, including visceral fat loss.
Early real-world research reported in 2025 suggests women using tirzepatide may lose more weight when they’re also on menopause hormone therapy, compared with tirzepatide alone. This is promising, but it still needs careful medical follow-up.
If you go this route, protect your muscle with protein and strength training, or you can lose more than fat.
A clear next-step checklist to discuss with your HRT specialist in Chicago
Bring these to your appointment:
- A symptom list (hot flashes, sleep, mood, vaginal dryness, joint pain)
- Your weight trend and waist measurements (even just 4 to 8 weeks)
- A quick snapshot of what you eat and how you move
- Meds and supplements
- Family history (clots, stroke, breast cancer)
- Your goals (symptom relief, Weight Loss, strength, energy)
Questions to ask:
- Which type and route of HRT fits your history best (patch, pill, gel, other)?
- How will you monitor side effects, blood pressure, and symptoms?
- What changes are realistic in 8 to 12 weeks?
- What should you do if bloating or scale changes show up?
It also makes sense to ask if you should check common contributors like thyroid labs, A1C, lipids, and blood pressure based on your clinician’s guidance. For local support, Managing Menopause Symptoms with Professional Help can help you plan what to address first.
Conclusion
Menopause can shift fat toward your belly, even when your habits haven’t changed much. HRT can help slow visceral fat gain and remove barriers like poor sleep and low energy, but it won’t replace food quality, strength training, daily movement, and stress care. The most reliable path to Weight Loss in midlife is steady: protect muscle, maintain a modest calorie gap, move daily, and lift consistently. Bring your symptoms and your goals to a qualified clinician, then build a plan that fits your body and your life in Chicago.
